On December 22, I had arthroscopic surgery on my right knee. I was diagnosed with a tear in the medial meniscus cartilage. Here’s a diagram of what that means.
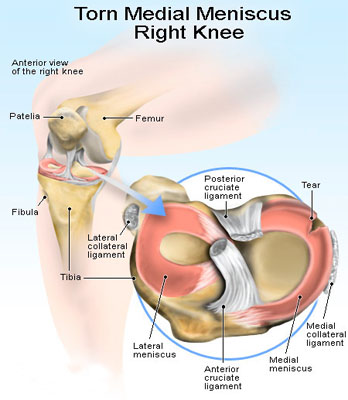
The tear was diagnosed by an MRI. Unlike the diagram, my tears appeared to on the inside edge of the cartilage, not the outside. In addition to the meniscus tear, I was also diagnosed with osteoarthritis, which showed up as “fuzziness” in the surface cartilage in the tibia and femur in x-rays.
I was under general anesthesia for the operation which took less than an hour. Three small incisions were made to introduce the camera, light source and surgical instruments.
Here are a couple picture of the inside of my knee showing the torn (frayed really) menicus cartilage. The stuff that looks like fringe is the torn up inner edge of the cartilage.
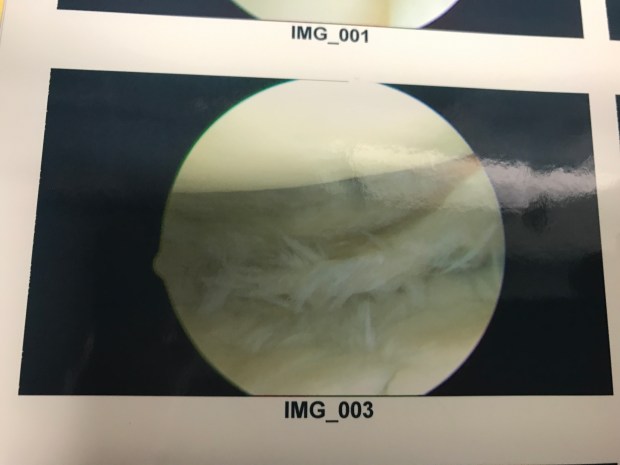

There were also some pictures of the meniscus after the repair, but I didn’t manage to take photos of that. The doctor also showed me pictures of the surface cartilage where it was degraded from the arthritis. He said it was likely that this will potentially get worse over time, but could be treated with cortisone, simvisc and stuff like that.
I asked him if I should avoid impact sports like running. He said that the research was inconclusive and contradictory. He advised me to go by how the joint felt. If it started to hurt, then avoid running. I asked if I was OK to start rowing again and he gave me the green light for that.
After the surgery, I recovered quickly. I was on crutches for a day. I kept it iced during the day over the first 2 days, and it was basically immobilized with an ace bandage for four days. After 4 days, I took off the ace bandage and changed the little bandages on the incisions daily. I was walking a little stiffly on day 4, but gradually increased the range of motion of the knee. By day 6, the range of motion was just about normal. The only time I felt a twinge was walking down stairs. I found out later that this is likely to be related to the osteoarthritis, not the meniscus and I should just get used to it.
I didn’t have any trouble with pain. The doctor prescribed over the counter anti-inflammatory (Ibuprofen) to minimize swelling and I took that constantly for the full 10 days until the follow up appointment. I did not need to take any of the stronger painkillers that he gave me.
And now I’m back at it. Yesterday’s CTC session was slower than I liked, but that’s due to a lack of fitness, not a knee problem. This morning, after rowing hard at r28, I have no knee pain or swelling. I’m ready to call the surgery a success.